Feasibility and safety report on robotic assistance for cervical pedicle screw fixation: a cadaveric study

Specimen preparation
Three freshly frozen human cadaveric specimens from the C2-T3 region were used. All specimens underwent thorough visual inspection to ensure the absence of fractures, deformities, prior surgery, or severe spondylosis.
A CT scan was performed for all specimens (120 kV, 20 mA, 0.62 mm; GE Brightspeed, Boston, MA) to assess bone quality and obtain measurements for planning the ideal implant size and pedicle screw trajectory.
This study was approved by the Yonsei University Health System Ethics Committee IRB (‘Single-institution, prospective researcher-led exploratory clinical study to evaluate clinical efficacy and safety of CUVIS-SPINE, navigation medical stereotaxic device’ 1-2020-0025). The clear source of cadavers were adhered in the laboratory of the Korean Surgical Robot Education Center, through the Department of Anatomy at Yonsei University College of Medicine.
Surgical instrumentation and technique
The cadaveric specimen was placed in the prone position on the surgical table, with the head stabilized using a Mayfield head clamp (MHC, manufactured by. Ohio Medical Instrument Co., Cincinnati, Ohio). The lower cervical spine was maintained in a neutral position. The surgical procedure involved using the CUVIS Spine robot developed by CUREXO and a long-arm screw manufactured by GS Medical. The necessary equipment for surgery included an intraoperative C-arm scan combined with CUVIS Spine navigation and robotic assistance provided by CUREXO (Seoul, Korea). The operating room settings are shown in Fig. 1.
The posterior neck area was prepared meticulously, including shaving, scrubbing, and draping, to ensure a sterile environment. The patient reference array was securely attached to a two-pin fixator, which was connected to a Mayfield holder and positioned adjacent to the surgical field. The CUVIS Spine Robotic System was positioned on the left side of the operating room table. Once the C-arm scan was completed in both the anteroposterior and lateral views with minimal motion artifacts, the captured images were automatically transferred to the CUVIS Spine navigation system for digital reconstruction and registration using preoperative spine CT scans.
Navigation tools were integrated into the system with types of arrays which attached at robot body and arm, and a navigated probe was used to determine the optimal entry point for the procedure. A median skin incision was made to expose the spinous process and laminae at the target level. The CUVIS Spine Robotic System was aligned and securely fastened along the desired trajectory for screw placement. Utilizing a 1.5-mm diameter navigated drill guided by image assistance, a pilot hole was created in the dorsal cortex of the left lateral mass through the cannula attached to the robotic arm. Tapping and insertion of the Long-arm Pedicle Screw System (GS Medical (23263 Madero Suite C Mission Viejo, California 92691, US)) were performed through the pedicle.
Screw diameter and length were determined perioperatively with the assistance of image guidance under the supervision of a senior surgeon. The same procedure was performed on the patient’s right side. A subsequent C-arm scan was performed intraoperatively to assess implant positioning. Upon confirmation of satisfactory implant positioning, the system was securely locked, and any attachments, such as the long-arm wing, were removed using a wing holder.
These procedural steps, involving the use of the CUVIS Spine robot by CUREXO and the long-arm screw provided by GS Medical, in conjunction with advanced imaging and navigation technologies, enable precise and accurate fixation of posterior cervical pedicle screws. Intraoperative C-arm images were acquired using a C-arm scanner and were transferred to a workstation. Based on these images, the spine surgeon planned the entry point, angle, and depth of the pedicle screw and determined its characteristics (Fig. 2a). The planned path was overlaid on the intraoperative C-arm image, and the robotic arm was targeted to the planned path, allowing the surgeon to insert a screw (Fig. 2b–d). Integration of these technologies and techniques facilitates a minimally invasive approach that can improve patient outcomes and reduce surgical invasiveness.
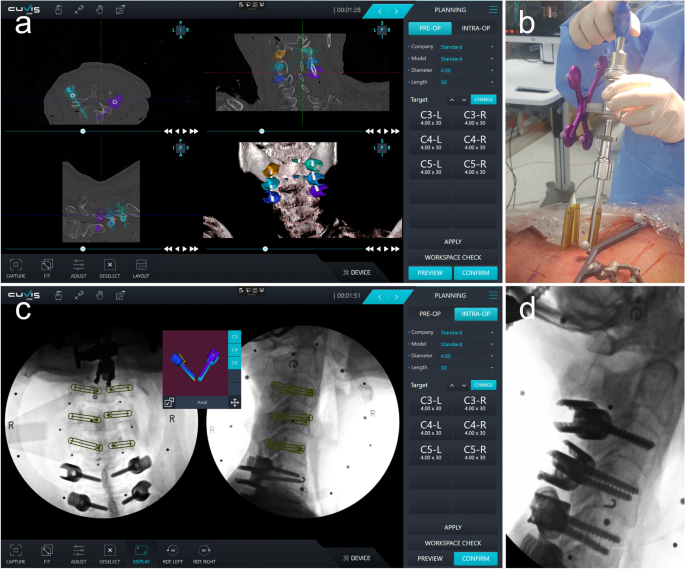
Procedures of robot-assisted posterior cervical pedicle screw insertion. (a) Preoperative CT-based planning of pedicle screw trajectory. (b) Robot-assisted pedicle screw placement. (c) Planned path overlaid on an intraoperative C-arm. (d) C-arm lateral image of cervical pedicle screw insertion.
The specification of CUIVS-spine
CUVIS-spine consists of a robotic arm with a 5-degree-of-freedom manipulator, a main console including a 3D position measurement camera and a user monitor, and a staff console including an auxiliary monitor for the user. The manipulator consists of 2 to 5 axes, including 1 axis that performs linear motion in the forward and backward direction with 5 total degrees of freedom, and a rotation axis.
The Size and Weight were as follow. Robotic Arm : 602 × 648.5 × 1 072 (mm), 266 (kg), Main Console : 040–2340 × 650 × 728 (mm), 78 (kg), Staff Console : 1346 × 650 × 728 (mm), 32 (kg). Pose repeatability are position error ≤ 1.00 mm, orientation error ≤ 1.00°, and Pose accuracy are position error ≤ 1.00 mm, orientation error ≤ 1.00°. The Optical Tracking System (VEGA; NDI) and Target Tracking are operational.
Accuracy evaluation
Postoperative CT images were used to assess the accuracy of pedicle screw placement in this cadaveric study involving 40 screws. In previous studies, the Gertzbein-Robbins classification system (GRS) was commonly employed to evaluate the accuracy of pedicle screw placement12,13,14,15. However, owing to the inherent differences in the spinal structure between the lumbar, cervical, and upper thoracic regions, applying the same criteria for accuracy evaluation in this study was challenging. Consequently, we adapted the Neo classification system for cervical pedicle screws to assess the accuracy of pedicle screw placement16,19. The evaluation involved categorizing the clinical grades into two groups: acceptable, defined as a grade of ≤ 1 for the Neo classification, and poor, indicated by a grade > 2 (Supplementary Fig. S1).
Although the GRS is useful, it lacks quantitative measures, and its limitations make comparing data across various experiments challenging. Consequently, there is a need for a quantitative measurement method that allows comparison with other datasets. To address this issue, the following evaluation criteria were utilized: entry offset, target offset, and angle offset, which were calculated based on postoperative CT images (Fig. 3).
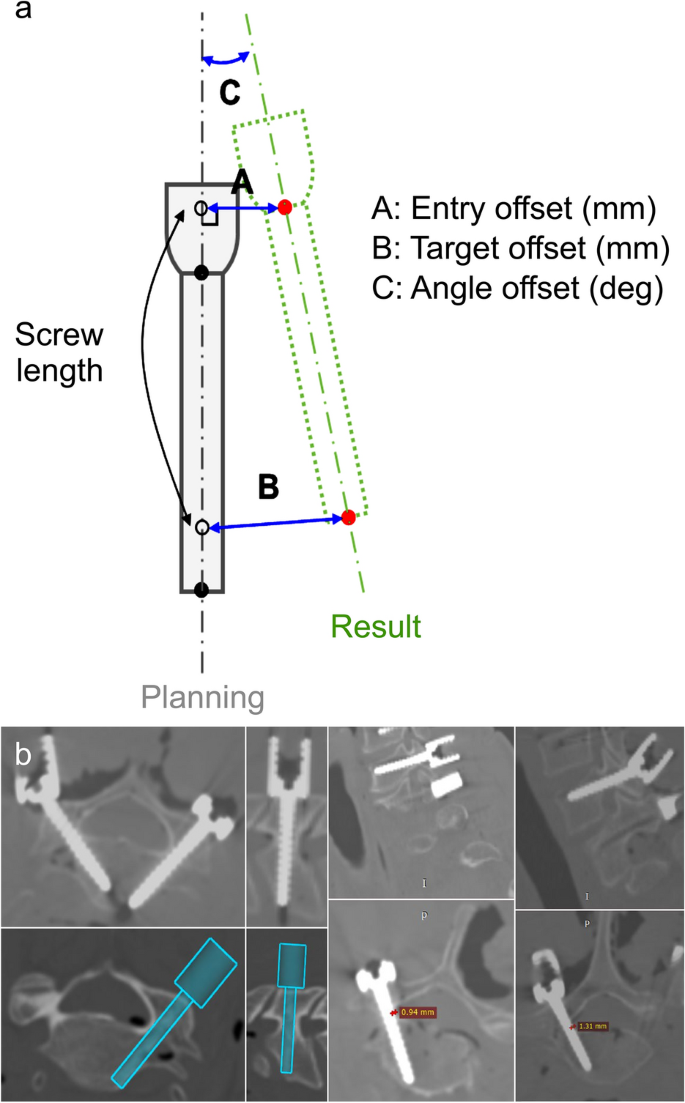
Measurement of the accuracy of robot-assisted posterior cervical pedicle screw insertion. (a) Definitions of three offsets, entry offset (mm), target offset (mm), and angle offset (deg.), between the planned and postoperative paths. (b) CT-based measurements of offset and cortical breach.
Quantitative measurements were performed using CT scans for the 3D assessment of the accuracy of the screw tip, screw tail, and screw angulation. Image overlay analysis was performed to compare the planned trajectories prior to surgery with the actual post-surgery screw placement. The 3D accuracy assessment was documented for the anterior-most part of the screw (tip), posterior-most part of the screw (tail), and mean accuracy value. The angular offset was determined by calculating the difference in the angle between the vectors of the planned and placed screws20.
Additionally, the GRS, Neo, and Heary grades were used for postoperative accuracy analysis19,21. However, technical issues concerning file compatibility, trajectory file processing, and image analysis impede postoperative accuracy analyses in some instances. To ensure unbiased evaluations, all assessments were conducted independently by a blinded robotic engineer and neurosurgeon.
Statistical analysis
Descriptive statistics for continuous variables are reported as mean ± standard deviation.
A comparative analysis was conducted juxtaposing the results of this study with those of previous studies that employed two distinct robotic systems for cervical and upper thoracic pedicle screw fixation. These studies functioned as comparative benchmarks for evaluating screw placement accuracy. The precision of screw placement was determined by calculating the percentage of screws positioned within predefined safe zones based on established guidelines and anatomical considerations. Identical criteria and parameters were applied to all three robotic systems to ensure consistency and comparability. To compare the accuracy grading between the domestically developed robotic system and the two previously studied systems, Fisher’s exact test was conducted with the significance level set at p < 0.05. All statistical analyses were performed using SPSS version 26 (IBM Corp., Armonk, NY, USA).
Ethics declarations
This study was approved by the Yonsei University Health System Ethics Committee IRB (‘Single-institution, prospective researcher-led exploratory clinical study to evaluate clinical efficacy and safety of CUVIS-SPINE, navigation medical stereotaxic device’ 1-2020-0025). The authors can confirm that all the methods employed in our research were carried out in full accordance with the appropriate guidelines and regulations in Scientific Reports.
Approval for human cadaveric experiments
Approval for human cadaveric experiments was obtained through the Korea Surgical Robot Training Center and Yonsei University Health System Ethics Committee IRB.
Consent to participate
The requirement for informed consent was waived by the Korea Surgical Robot Training Center and Yonsei University Health System Ethics Committee IRB since all participants in this study were cadavers.



